Etiology & Epidemiology
Introduction to HIV and AIDS
What is HIV?
HIV is an acronym for Human Immunodeficiency Virus—an infectious disease that damages the immune system, and in turn, decreases the body’s ability to fight off other diseases and infections effectively. First discovered in 1983, this life-threatening infection has spread at an astounding rate affecting people across the globe.
According to the World Health Organization (WHO), it was estimated that by the end of 2015, approximately 36.7 million people were living with HIV worldwide. The CDC (Centers of Disease Control & Prevention) estimated that approximately 44,073 people were living with HIV in the United States by the end of 2014. This is actually a decline by 19% from 2005-2014, which was possibly due to high efforts in preventing HIV. In Washington State alone at the end of 2014, 12,500 people were living across the state with HIV (DOH 2015, 2nd ed.).
As of yet, there is no cure for HIV. It can be controlled however. With the proper administration of antiretroviral therapy drugs (discussed later) and continuing prevention practices, an infected HIV person can prolong their life dramatically.
Once a person gets HIV, they have it for life. HIV in its highest form is AIDS.
What is AIDS?
AIDS is short for Acquired Immunodeficiency Syndrome and is representative of the advanced and third stage of HIV—the most threatening level when cells are impaired or simply die in the immune system at a progressive rate. By this time, other infections and diseases have attacked the body causing it to struggle even more.
When the immune system is “deficient” of its normal functioning, people become much more vulnerable to disease and infection by organisms such as bacteria and viruses. Thus, in the advanced stages of HIV, many infected with the virus contract a number of new infections, creating a more complexed condition.
When HIV evolves into a multitude of diseases and infections, the disease is labeled as AIDS. This means that a group of symptoms are occurring together, and such grouping of symptoms is referred to as a “syndrome.”
AIDS is an acquired disease and the only way to be infected is by the infection entering the bloodstream. It is not hereditary, nor is it passed by casual contact with another person.
Compared to its peak year in 2005, AIDS-related deaths dropped 45% by the end of 2015 (UNAIDS, 2016). However, the number was still enormous. In 2015, 1.1 million people died from AIDS-related causes worldwide.
Antiretroviral drugs (ART) was introduced in the mid-1990s as a means to treat HIV. Prior to that, people could progress to AIDS in just a few years. If an infected HIV person is diagnosed early enough and treated before the disease is far advanced, one can live nearly as long as someone who doesn’t have HIV.
The Infection In Action
How HIV Attacks:
HIV is a blood-borne pathogen that must have access to the bloodstream for a person to be infected. When HIV enters the bloodstream, it zeros in on white blood cells called lymphocytes—cells essential to fight off disease- causing organisms such as viruses and bacteria. These cells are often referred to as “T-Helper lymphocytes” and are sometimes called T, T4, or CD4 cells. If an HIV infected person goes untreated, the number of CD4 cells reduce in the body.
Along with this reduction of lymphocytes, the production of antibodies reduce as well. Antibodies (also known as immunoglobulins) are blood proteins produced in the immune system by lymphocytes. They play a major role there and have the ability to terminate foreign invaders that attack our bodies, like the measles and polioviruses. They are our pathogen destroyers and bind directly with intruders to prevent them from damaging our healthy body cells. In the case of an HIV infected person, whose immune system isn’t working properly, the ability to create sufficient antibodies to fight off infection becomes severely diminished.
After a period of time, these T-Helper lymphocytes are very few in the immune system, and antibodies just as few, and the risk of getting “opportunistic” infections or cancers increases. Once those other infections start to double up, then triple, advanced HIV signals in, or rather the stage known as AIDS.
How HIV is Classified:
When a person is a confirmed case of HIV, there are actually five stage classifications (Stage 0, 1, 2, 3, and Unknown), yet there are only three main stages that can measure the important CD4 cell count—the determining factor for HIV progression.
A CD4 count is measured as the number of cells in a cubic millimeter of blood. A normal range usually falls between 500 to 1,500 cells per cubic millimeter of blood. The pattern of results are more important to evaluate than the result of any one test when testing for HIV, and the disease is generally said to be progressing if the CD4 count is decreasing.
When a person has been diagnosed with HIV and has a negative HIV test within 6 months, that person is considered to be in a Stage “O” of HIV until six months has passed from their first diagnosis.
Window Period
- This describes the time period between the first initial point of HIV infection to the point when antibodies to HIV can be detected in the body
- It’s during this window period that antibodies have not had a chance to produce in sufficient amount, meaning the person might get a negative result when taking an antibody test and yet be positive with the virus.
- Even though the antibodies have not developed for testing, an HIV infected person will have a large amount of virus in their body. This means they are contagious and can transmit the virus.
- Sometimes it takes up two weeks to three months for the development of antibodies to show up on lab tests.
- Antibodies for HIV normally appear within six weeks for most people.
- New, advanced testing has recently become available that shortens this window period and has provided newly infected people a chance to learn of their status sooner and receive the necessary medical treatment that can control HIV. In doing so, the virus becomes less infectious and health is prolonged.
The Main Stages of HIV:
Stage 1 – Primary/Acute HIV Infection
- The virus establishes itself in the body, sometimes causing sickness that typically last only a week or two.
- Symptoms are usually flu-like in nature and may develop within 2 to 4 weeks after HIV infection.
- Some people have little to no sickness and may not be aware they are infected.
- The term “acute HIV infection” is often used by clinicians to describe the period between when a person is first infected with HIV to the point when antibodies against the virus are able to be detected by an HIV test.
- This is a very contagious period as there is a large amount of infection in the blood at this time.
Stage 2 – Chronic HIV Infection / Clinical Latency
- Sometimes referred to as the Asymptomatic Stage as people tend to be sick-free and can look and feel fine for ten years or longer, even being untreated.
- Although the disease appears to be latent, it is during this time that the virus is replicating and destroying T4 cells, as well as seriously damaging the immune system.
- The disease can easily be transmitted to another person though unprotected anal, vaginal or oral sex or via needle sharing at this time.
- The virus can be transmitted from an infected mother to her unborn child, through childbirth or through breastfeeding.
- The importance for treatment through drugs and HIV prevention methods are vital (as with the Acute Stage). By taking antiretroviral medications, an infected person can reduce their chances of transmitting HIV to another person by more than 90%.
- At the end of this stage, the CD4 count drops and the viral load (virus level in the body) increases.
Stage 3 - Acquired Immunodeficiency Syndrome (AIDS)
- By this time, the immune system is overly damaged and an increased number of illnesses sneak in, other diseases causing a multitude of health problems.
- Without treatment, the lifespan of an AIDS person is about 3 years.
- Symptoms may include fatigue, rapid weight loss, chills and profuse night sweats, swollen lymph glands, recurring fevers, sores in
- the mouth, anus, and genitals, memory loss and depression. Diagnosis of AIDS is determined by CD4 cell counts dropping below 200 cells/mm or the development of opportunistic illnesses. These are infections or cancers occurring due to an impaired immune system. Examples of opportunistic infections that might arise are Kaposi’s Sarcoma, Toxoplasmosis, or Cytomegalovirus. The most common and a leading cause of death for the HIV-infected person is Pneumocystis Pneumonia (PCP).
When test results do not coincide with the first, second and third stages of HIV, such as missing information from the CD4 test results, the stage of HIV is considered “Unknown.”
How HIV Began:
The origin of HIV was not discovered for more than a decade following the first case of HIV. Researchers from all over the world teamed up to find the virus’ original source and in 1999, reported their findings. They found that HIV 1—the predominant strain of HIV—originated in a subspecies of chimpanzees living in west equatorial Africa. Theory has it that hunters were first introduced to the virus when exposed to the infected blood. Later, through genetic information, the virus was further traced to have passed to its first human being within the first two decades of the Twentieth Century.
The spread of HIV has since migrated due to travel, warfare, sexual practices, drug use, and a variety of other economic movement affecting on a global level.
First cases of HIV:
Although HIV is said to have started in the United States in the 1980s, the fact is, the U.S. only became aware that the fatal infection existed. It was then that a new health condition was officially recognized.
The first cases of rare diseases began showing up in 1982, and these were among gay men in New York and California. Such diseases as Kaposi's Sarcoma (a rare cancer) and a lung infection called PCP (PneumocySTIs Carinii Pneumonia) began revealing themselves on tests. Why these cancers and opportunistic infections were spreading, no one knew.
The disease was first labeled by people with all sorts of names relating to the word “gay.” Around mid-1982, it was realized that the infection was spreading quickly and among other populations, such as hemophiliacs and heroin users. In September of 1982, the term “AIDS” was born.
Different Strains of HIV:
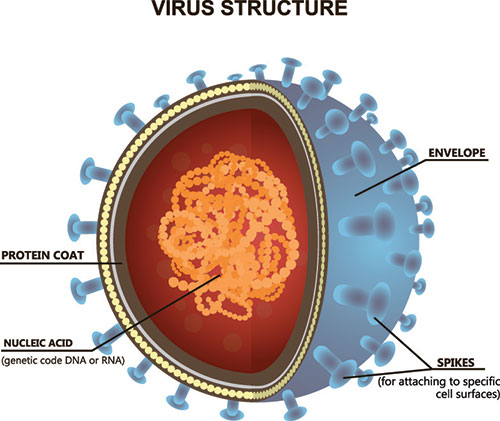
There are numerous strains of HIV as this highly variable virus mutates readily and rapidly. One person infected with HIV can have several types of strains within their body. Classified into types, groups and subtypes, the two primary strains are HIV-1 and HIV-2. HIV-2 is not as common a strain and mainly concentrates in West Africa. In fact, it has rarely been found elsewhere.
HIV-1, the major strain worldwide, is specified as HIV for the general virus. Both primary strains are transmitted through blood and other bodily fluids that are HIV friendly (semen, vaginal and cervical secretions, rectal secretions and breast milk). HIV-1 and HIV-2 both cause AIDS.
As each strain has several subtypes, the probability for more HIV subtypes to evolve is high. HIV testing is presently capable of detecting all known subtypes of HIV, as well as the two primary strains.
Who is at Risk?
The study of incidences and the distribution of disease in populations throughout the world is called epidemiology. Included in such research is discovering the influencing factors behind a disease and controlling it before it becomes too incontrollable. One area of study for the epidemiologist is to seek out answers as to why a disease is prominent in some groups more so than others are.
In 1981, the first case of AIDS was recognized in the United States. The first report of AIDS in Washington State happened in 1982. The number of cases have devastatingly increased with rapid speed. HIV has proven to have no bounds and people of all races, ethnic backgrounds, genders, and income levels have contracted the disease. Exposure to the virus can infect anyone through occupational or non-occupational risks. There are geographical areas in the world where HIV disease is projected in greater numbers, and as with any disease, certain other factors can significantly raise one’s risks for getting HIV.
Regional Statistics:
The U.S. Centers for Disease Control and Prevention (CDC) estimates that an American has a 1 in 99 chance of contracting HIV in their lifetime. That risk is raised for those living in the South. Other areas at highest risk in the U.S. include Washington D.C., followed by Maryland, Georgia, Florida, Louisiana, New York, Texas, New Jersey, Mississippi, South Carolina, North Carolina, Delaware, and Alabama.
According to the Washington State HIV Surveillance (2015b), greater than 20,000 people thus far have been diagnosed with HIV in Washington State with more than 6,700 deaths resulting from HIV disease. On a recent note, new HIV cases have decreased in Washington State slightly. New cases averaged at 492 per year between 2010 and 2014.
The most affected region on a global scale is sub-Saharan Africa, where approximately 25.6 million people live with HIV (2015 statistics). This region also accounts for two-thirds of the global total of new HIV infections.
Today, with 36.7 million people living with HIV worldwide, as of June 2016, only 17,000 are receiving antiretroviral therapy to treat HIV. Often diagnosed through rapid diagnostic tests (RDTs) that reveal the presence or absence of HIV antibodies, people can now receive results in the same day, which is vital for early diagnosis so that treatment and care can begin as soon as possible. It is through these improved prevention methods that have assisted in lowering the disease’s fatality rate.
New HIV Diagnoses by Race / Ethnicity

HIV-Infected Unawareness:
It is estimated that one in ten people living in Washington State are unaware they have the virus. In the whole of the United States, that ratio of unawareness extends up to a quarter of the population in the country. That means that people have not been tested for HIV. Nor do they realize they have the infection and can transmit it to others. As stated previously, symptoms of newly infected people may or may not have symptoms, or will present only flu-like symptoms for a brief time. Afterwards, people infected can look and feel completely well for as long as a decade. Yet infection is dangerously contagious during this latent/asymptomatic period.
Reporting HIV & AIDS
HIV cases are reportable to the Washington State Department of Health and have been required since the fall of 1999. AIDS cases have been reportable since 1984. For more in-depth information about the legal requirements of reporting HIV & AIDS, see Section 5 of this course.
Contact the Washington State Department of Health at (360) 236-3444.
For updated information on reported HIV & AIDS cases in Washington State, visit: http://www.doh.wa.gov/
Case Report forms are available on the health department's disease reporting webpage.
Visit these websites for current HIV and AIDS statistics:
http://www.doh.wa.gov/cfh/hiv.htm
http://hivinsite.ucsf.edu/
http://www.cdc.gov/
http://www.unaids.org
Purpose of reporting disease:
- Gathering information about infected people helps toward creating programs that will prevent the disease.
- Those who are infected can be referred to medical care immediately.
- Identifying infected people provides a means to stop the spread of infection.
Confidentiality
The identity of persons reported to have HIV or AIDS are protected by state laws. Breaking these laws may result in legal repercussions and large fines. Records belonging to HIV infected people have a higher level of protection than other health records. To have access to these records, one must be a health provider of HIV medical care or authorized person, and the use of information must be used for a specific public health purpose. Physical and electronic records are protected to prevent them from being improperly disclosed. Special training as to how they are to be safeguarded is given annually to those who have access to them.